
If I’m thinking about LASIK, corneal topography is one of the first tests that can help show whether it’s safe for me. It maps the shape and thickness of my cornea, helps spot early signs of keratoconus or other shape problems, and can lower the risk of post-LASIK ectasia.
Here’s the short version:
- Topography maps the front of the cornea
- Tomography adds the back surface and thickness data
- LASIK is often avoided if the cornea is too thin, too steep, or uneven
- A PTA under 40% is linked with lower ectasia risk
- Posterior elevation, pachymetry, and map pattern overlap matter a lot
- Soft contacts usually need to be out for at least 1 week before testing
- If LASIK looks risky, PRK or corneal cross-linking may be the safer next step
A few numbers often reviewed during screening:
- Central corneal thickness: over 500 µm may support LASIK
- Posterior elevation: +17 µm or less is often more reassuring
- Mean keratometry: above about 47.2 D to 48.7 D may be a warning sign
- Thickness gap: more than 27 µm between central and thinnest point can point to very high ectasia risk
What this means for me is simple: LASIK is not just about my glasses prescription. It’s also about whether my cornea can stay stable after tissue is removed. Surgeons look at curvature, elevation, thickness, and risk scores together – not one map by itself.
| Test area | What it helps show | Why I should care |
|---|---|---|
| Curvature map | Steep and flat areas | Finds astigmatism patterns and uneven shape |
| Elevation map | Front and back bulging | Can spot early back-surface changes |
| Pachymetry map | Corneal thickness across the eye | Helps show if enough tissue will remain |
| Risk scores | Hidden keratoconus risk | Adds another check before surgery |
So before LASIK moves forward, this scan helps answer the big question: is my cornea a safe match for laser reshaping?
Corneal Topography Pearls: Kanellopoulos, MD
sbb-itb-c87b093
How Corneal Topography Works in a LASIK Evaluation
Topography is just one part of the LASIK safety check. Surgeons look at it along with refraction, tear film analysis, pupil measurements, pachymetry, and a dilated retinal exam. From there, they use different imaging tools to get a close look at the cornea.
Imaging systems used by surgeons
Before LASIK, surgeons usually rely on two main ways to image the cornea: Placido-disc topographers and tomography devices.
Placido-disc systems project concentric rings onto the tear film and study how those rings reflect back. This method maps only the front surface of the cornea.
Corneal tomography looks deeper. Devices such as Pentacam, Orbscan, and Galilei capture the front surface, back surface, and corneal thickness in one scan. That 3D view matters for LASIK screening because it can show subtle changes on the back surface of the cornea before those changes appear on the front.
What patients experience during the test
The test is painless and usually takes only a few minutes. You place your chin and forehead on the device, stare at a target light, and stay still while the camera captures the scan.
There’s one part patients often overlook: contact lenses. Soft lenses should be removed at least 1 week before the exam, and rigid gas-permeable lenses need to be out for several weeks. If they’re worn too close to the visit, they can warp the cornea, distort the map, and throw off the LASIK evaluation.
The main maps reviewed before LASIK
Surgeons usually review four map types when checking whether someone is a good LASIK candidate:
| Map Type | What It Shows | Why It Matters for LASIK |
|---|---|---|
| Axial / Sagittal | Overall corneal curvature and power | Shows overall curvature and common astigmatism patterns |
| Tangential | Localized slope and curvature at specific points | Shows small, localized irregularities |
| Elevation | Corneal height compared to a reference sphere | Shows subtle front- or back-surface bulging |
| Pachymetry | Thickness distribution across the entire cornea | Shows corneal thickness and whether enough tissue remains for LASIK |
Taken together, these maps show the cornea’s shape, thickness, and any hidden irregularity. Those details feed straight into the approval criteria surgeons review next.
What Surgeons Look for Before Approving LASIK
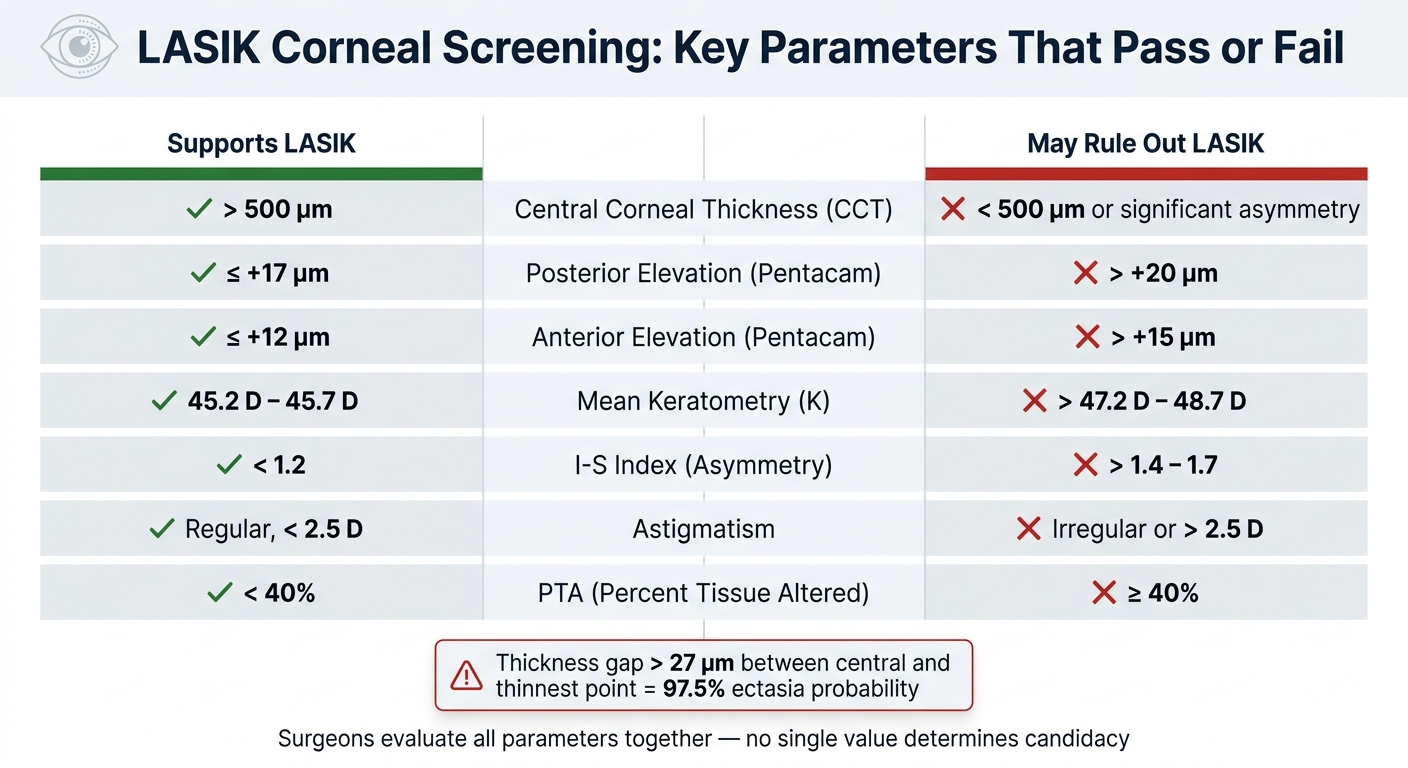
LASIK Corneal Screening: Key Parameters That Pass or Fail
With the maps in front of them, surgeons look for one big thing: can the cornea handle reshaping without slipping into ectasia?
Normal findings that support LASIK candidacy
The first step is pretty straightforward. The surgeon checks whether the cornea appears strong and steady enough for laser treatment. In most cases, a good LASIK candidate has enough corneal thickness, stable refraction, similar map patterns in both eyes, and regular astigmatism.
One number surgeons watch closely is Percent Tissue Altered (PTA). This figure uses flap thickness, ablation depth, and central corneal thickness. A PTA below 40% is strongly linked with a lower risk of post-LASIK ectasia.
Refraction should also stay stable for at least 12 months before surgery is considered.
| Parameter | Supports LASIK | May Rule Out LASIK |
|---|---|---|
| Central Corneal Thickness (CCT) | > 500 µm | < 500 µm or significant asymmetry |
| Posterior Elevation (Pentacam) | ≤ +17 µm | > +20 µm |
| Anterior Elevation (Pentacam) | ≤ +12 µm | > +15 µm |
| Mean Keratometry (K) | 45.2 D – 45.7 D | > 47.2 D – 48.7 D |
| I-S Index (Asymmetry) | < 1.2 | > 1.4 – 1.7 |
| Astigmatism | Regular, < 2.5 D | Irregular or > 2.5 D |
| PTA (Percent Tissue Altered) | < 40% | ≥ 40% |
Red flags that may rule out LASIK
The same maps that support LASIK can also show early warning signs.
Forme fruste keratoconus is the most important risk factor for post-surgical ectasia. It often appears as localized steepening on the curvature map, along with subtle posterior elevation changes before anything shows up on the front surface. That’s why back-surface data matters so much. Trouble can start there first.
Pellucid marginal degeneration has a different look. It often shows a "crab-claw" or butterfly steepening pattern in the lower outer cornea. If that cornea is thinned more with a laser, the risk of severe structural instability goes up.
Thickness patterns matter too. When the gap between central thickness and the thinnest measured point is more than 27 µm, the probability of ectasia is 97.5%.
| Risk Factor for Ectasia | What Topography or Tomography Can Detect | Why It Matters |
|---|---|---|
| Forme Fruste Keratoconus | Localized steepening (often inferotemporal) and posterior elevation | Most significant risk factor for post-surgical ectasia |
| Pellucid Marginal Degeneration | "Butterfly" or "crab-claw" steepening in the inferior periphery | Leads to severe corneal instability if thinned further by laser |
| Thin Residual Stromal Bed | Calculated by subtracting flap thickness and ablation depth from CCT | Insufficient residual stromal bed can lead to structural failure and bulging |
| Abnormal Posterior Elevation | "Island" or "ridge" patterns on posterior elevation maps | Suggests early back-surface bulging before anterior changes appear |
| Contact Lens Warpage | Topographic steepening with epithelial thickening | Can mimic ectasia; requires a lens holiday before accurate mapping |
When a different treatment may be safer
If the maps sit in a gray area, the next step is not to push ahead with LASIK. It’s to pick the option that leaves more corneal strength in place.
Borderline or abnormal maps do not rule out vision correction. They rule out LASIK. PRK is often the safer pick for people with thinner corneas or mild structural concerns because it reshapes the surface without making a flap, which leaves more support behind.
If screening points to an ectatic process, corneal cross-linking may come first to help stabilize the cornea before surgery is considered.
How to Read Corneal Maps and What They Show
Once the maps are done, surgeons read them together, not one by one. The big idea is alignment. If the steepest point on the curvature map, the highest point on the elevation map, and the thinnest point on the pachymetry map all show up in the same spot, that overlap matters more than any single finding by itself.
On most maps, warm colors like red, orange, and yellow mark steeper or higher areas. Cool colors like blue and green mark flatter or lower areas. Pachymetry is the exception: cool colors mean thicker tissue, while warm colors mean thinner tissue.
Curvature, elevation, and pachymetry maps explained
The curvature map shows front-surface steepness and power in diopters. The pattern matters more than one isolated number. A symmetric bowtie usually points to regular astigmatism. An asymmetric bowtie, a "lazy C", or a broken bowtie pattern can suggest irregular astigmatism or early disease. That said, a normal front-surface pattern doesn’t rule out subtle changes on the back surface.
The elevation map compares the cornea’s actual shape with a mathematical reference surface called the best-fit sphere (BFS). In plain English, it shows where the cornea sits above or below that reference. The posterior elevation map gets extra attention because early ectatic changes often start on the back surface before they can be seen on the front.
The pachymetry map shows thickness across the whole cornea. Clear thinning can rule out LASIK. Surgeons also pay close attention to where the thinning is. For example, marked inferotemporal thinning can be an early sign of ectasia even when central thickness still looks okay. When shape and thickness sit in a gray zone, software scores can help put a number on the risk.
Software risk scores that help detect hidden risk
Modern imaging platforms calculate indices that can spot subtle abnormalities that may not jump out at first glance. BAD-D and KISA% are two common scores used to flag subtle keratoconus risk.
Table: What each map tells the surgeon
| Map Type | What It Shows | Why It Matters for LASIK Safety | Common Abnormal Findings |
|---|---|---|---|
| Curvature (Axial) Map | Surface power and steepness in diopters | Identifies astigmatism type and corneal regularity | Asymmetric bowtie or "lazy C" pattern |
| Elevation Map (Ant/Post) | Height of the cornea relative to a best-fit sphere (BFS) | Detects early bulging on the back surface before it appears on the front | Elevated posterior area or abnormal island/ridge pattern |
| Pachymetry Map | Full-surface corneal thickness | Ensures enough tissue remains after flap creation and laser reshaping | Marked thinning or significant inferior thinning |
| Advanced Indices | Software-calculated risk scores | Standardizes screening for subtle abnormalities | Elevated BAD-D or KISA% scores |
Corneal Topography Before, During, and After LASIK
Corneal topography helps guide LASIK from the first screening visit through follow-up after surgery. If the cornea clears screening, those same maps are then used for treatment planning and later checks.
The role of topography at each stage of LASIK
At the pre-op stage, corneal mapping checks whether the cornea is structurally safe for surgery. It can also spot hidden issues, including subclinical keratoconus, before they turn into a bigger problem. During planning, topography-guided LASIK uses that map data to treat irregular curvature and reduce aberrations such as coma and trefoil. At the post-op stage, mapping helps confirm centration, track the healing pattern, and watch for early instability.
| Stage | Topography Role | Key Questions Answered |
|---|---|---|
| Pre-op | Screening and baseline | Is the cornea thick enough? Are there hidden signs of disease? |
| Planning | Customized laser programming | How can the laser best address unique surface irregularities? |
| Post-op | Monitoring healing and stability | Did the cornea heal as expected? Are there any signs of ectasia? |
There’s one catch: those measurements only help if the cornea is in its natural state.
Patient factors that can affect test results
Good results depend on a stable corneal surface. Contact lenses can warp the map, which is why patients usually need a lens holiday before final measurements. Dry eye can also get in the way. If the tear film is unstable, the scan can give shaky data, so dry eye should be treated before final surgical measurements are taken. Even eye drops can matter. Dilating drops and other drops may temporarily shift pachymetry readings by about 17 ± 53 microns.
Key points patients should take away
The scan is fast, noncontact, and takes only seconds per eye.
FAQs
How do I know if my cornea is too thin for LASIK?
You’ll need a full pre-op exam, because corneal thickness is just one piece of LASIK eligibility. Ophthalmologists use corneal pachymetry to check whether there’s enough tissue for safe reshaping.
If your cornea is too thin, removing tissue can weaken the eye and increase the risk of problems like ectasia. At Boulder Eye Surgeons, doctors review these measurements alongside corneal topography and biomechanical assessments.
Can dry eye or contact lenses affect corneal topography results?
Yes. Dry eye can make corneal topography less accurate because the test relies on light reflecting off the tear film to map the cornea.
Contact lenses can affect the results too. They can temporarily change the shape of the cornea, which may throw off the imaging.
At Boulder Eye Surgeons, your ocular surface health may be checked before treatment planning to help make sure the images are accurate.
If LASIK is not safe for me, what other vision correction options are available?
If LASIK isn’t a fit, you may still have other paths based on your eye health and the shape of your cornea.
- PRK reshapes the cornea without making a flap.
- ICL is placed inside the eye and works without changing the cornea.
- RLE may be an option, especially for older patients.
Boulder Eye Surgeons can evaluate which option is right for you.



