
Pediatric cataract surgery is critical for preventing vision loss in children. Early intervention, ideally within the first 90 days of life, significantly improves long-term visual acuity. However, the journey doesn’t end with surgery. Children require ongoing care to address potential complications like glaucoma (affecting up to 41% of cases) and visual axis opacification (occurring in about 40% of pseudophakic eyes).
Key findings:
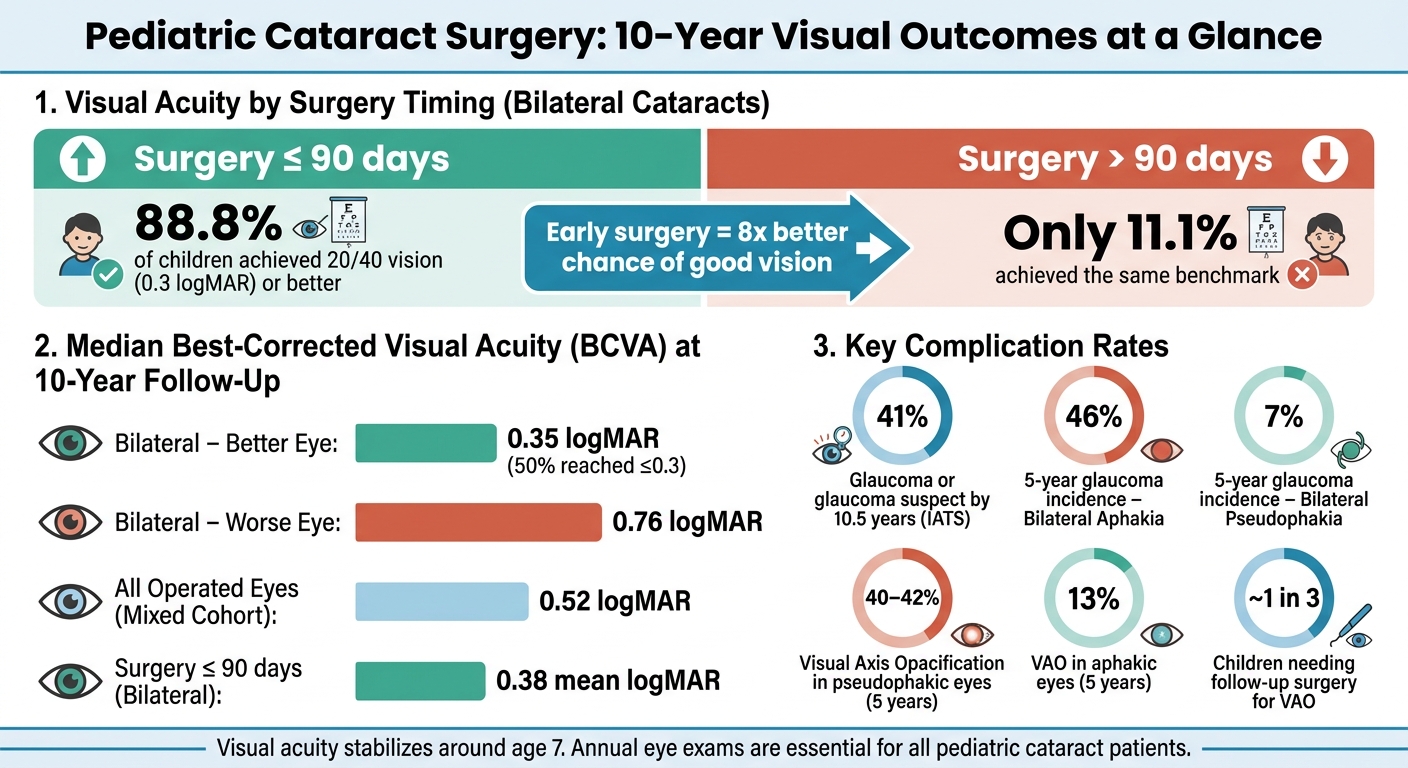
- Timing matters: Surgery before 90 days leads to better visual outcomes, with 88.8% achieving 20/40 vision or better.
- Glaucoma risk: Up to 46% of bilateral aphakic cases face glaucoma-related issues within 5 years.
- Post-surgery care: Regular follow-ups are essential to manage refractive changes and complications.
Parents and caregivers should prioritize early detection, timely surgery, and follow-up care to ensure the best outcomes for their child’s vision and quality of life.
Pediatric Cataracts and the Importance of Care
sbb-itb-c87b093
Study Population and Surgical Approaches
Long-term studies on pediatric cataracts focus on carefully selected groups to ensure reliable and consistent data. Researchers often exclude children with severe systemic conditions, such as Down’s syndrome or Marfan’s syndrome, to maintain compliance with vision testing protocols. This method helps create a focused group of participants, allowing for meaningful tracking of outcomes over extended periods. Below is a table summarizing key characteristics from major studies, which provides context for discussions on surgical timing and techniques.
| Study | Participants | Median Age at Surgery | Follow-Up Period |
|---|---|---|---|
| Mixed Uni/Bilateral – Denmark | 56 children | ~3 years (ranging from 42 days to 11.5 years) | Ages 7–18 at exam |
| Bilateral Dense Congenital – Sweden | 18 children | 52 days (range: 2–253 days) | Ages 10–18 |
| Unilateral Congenital – IATS | 112 children | 10.7 weeks (range: 4–30 weeks) | 10.5 years |
Patient Age at the Time of Surgery
The age at which surgery is performed varies significantly across studies, and this timing directly affects outcomes. For instance, the Infant Aphakia Treatment Study (IATS) reported an average surgery age of 10.7 ± 7.0 weeks for infants with unilateral cataracts, with some undergoing surgery as early as 4 weeks old. On the other hand, the Danish cohort exhibited a much broader range, reflecting the variation seen in clinical practice (as shown in the table). Within this group, children left aphakic had a median surgery age of 91 days, while those receiving primary intraocular lens (IOL) implants had a median age of 1,474 days.
Unilateral vs. Bilateral Cataracts
The approach to surgery and expected outcomes differ significantly based on whether the cataracts are unilateral or bilateral. Children with bilateral cataracts are generally operated on earlier, as highlighted by the Swedish cohort, where the median age at surgery was just 52 days. In these cases, the surgeries for both eyes are typically performed within a short interval – often just 2 days apart.
This distinction also impacts long-term outcomes:
"Children with unilateral disease often have a healthy eye to support the operated eye, why they overall have better subjective visual function." – Mathias Møller Hansen, Department of Ophthalmology, Rigshospitalet-Glostrup
In unilateral cases, the risk of deprivational amblyopia is higher in the affected eye. This often leads to earlier primary IOL implantation, typically after the child turns 1 year old. In contrast, for bilateral cataracts, surgeons often delay IOL implantation until the child is at least 2 years old.
Common Surgical Techniques Used
The surgical procedure involves several precise steps: creating a 2.4–2.75 mm limbal incision, performing anterior continuous curvilinear capsulorhexis (ACCC), bimanual lens aspiration, and posterior continuous curvilinear capsulorhexis (PCCC) . For children under 8 years old, a limited central anterior vitrectomy is also performed to prevent visual axis opacification and maintain clarity.
Over the past decade, IOL placement strategies have seen major changes. Surgeons are increasingly opting to implant a primary IOL even in younger infants – a practice that was once considered too risky.
"In the last decade, improvements in surgical technique, technology and better understanding of the growth of the eye have led to a more positive attitude among paediatric cataract surgeons to implant an IOL even in the youngest infants." – BMJ Open Ophthalmology
For infants younger than 6 months, surgeons often leave the eye aphakic and rely on contact lenses, postponing IOL implantation until the child is at least 4 years old . These refined surgical techniques play a critical role in shaping the long-term visual outcomes discussed in the next sections.
Visual Acuity at the 10-Year Follow-Up
Pediatric Cataract Surgery: 10-Year Outcomes by Timing & Lens Type
Best-Corrected Visual Acuity Results
A decade after surgery, visual acuity outcomes depend heavily on the type of cataract. For instance, a Swedish study focusing on bilateral dense congenital cataracts found that the median best-corrected visual acuity (BCVA) at the 10-year mark was 0.35 logMAR in the better-seeing eye and 0.76 logMAR in the worse-seeing eye. Roughly half of the patients achieved a BCVA of 0.3 logMAR (similar to 20/40 vision). Notably, visual outcomes stabilized around age 7 and remained steady through late adolescence.
In contrast, results from mixed cataract cohorts were less optimistic. A Danish study reported a median BCVA of 0.52 logMAR across all operated eyes. The outcomes varied significantly based on cataract type: 82% of children with unilateral cataracts had moderate to severe visual impairment, compared to 38% in those with bilateral cataracts.
| Patient Group | Median BCVA (logMAR) | Reached ≤0.3 logMAR |
|---|---|---|
| Bilateral – Better Eye | 0.35 | 50% |
| Bilateral – Worse Eye | 0.76 | N/A |
| All Operated Eyes (Mixed Cohort) | 0.52 | N/A |
| Surgery ≤ 90 days (Bilateral) | 0.38 mean | 88.8% (8 of 9) |
| Surgery > 90 days (Bilateral) | 0.57 mean | 11.1% (1 of 9) |
These figures highlight how both the timing of surgery and the type of cataract influence long-term vision, as explored further below.
How Surgery Timing and Cataract Type Affect Vision
The timing of surgery plays a pivotal role in determining visual outcomes. For bilateral cataracts, early intervention is critical. Surgery performed before 90 days of age led to significantly better results, with 88.8% of children achieving a BCVA of 0.3 logMAR or better. In stark contrast, only 11.1% of children who had surgery later reached this level. The Infant Aphakia Treatment Study (IATS), which tracked 114 infants over 10.5 years, reinforced this finding, demonstrating that the age at surgery strongly correlated with visual acuity at the 10-year follow-up.
"The major predictive factor for long-term visual outcome is age at surgery. Therefore, screening with early detection followed by surgery before the end of the third month is important to decrease the risk of marked acuity loss." – Acta Ophthalmologica
Cataract type also significantly impacts visual outcomes. Children with partial cataracts tend to fare better than those with total or dense cataracts, often achieving a mean visual acuity of 0.5 (decimal) by age 12. On the other hand, unilateral cataracts pose unique challenges due to deprivation amblyopia, which can hinder vision even when surgery is performed early. Interestingly, the IATS found no notable difference in 10-year visual acuity between children treated with a primary intraocular lens and those managed with contact lenses after unilateral surgery. This underscores that the timing of surgery is more influential than the method of vision correction used afterward.
"Chronological age was significantly associated with visual acuity at 10.5 years." – Infant Aphakia Treatment Study Group
Additionally, postoperative nystagmus substantially reduces the chances of achieving good visual outcomes, with affected children being 10.6 times less likely to attain favorable results.
Refractive Outcomes and Myopic Shift
Refractive changes play a key role in shaping long-term vision quality following pediatric cataract surgery, going beyond just visual acuity.
Refractive Changes After Surgery
After pediatric cataract surgery, eyes typically shift progressively toward myopia during the first decade, regardless of whether an intraocular lens (IOL) is implanted. However, the degree of this shift depends on the surgical approach.
Data from the IATS study shows that aphakic eyes experience a 44% reduction in refractive error between infancy and 10.5 years. Early in infancy, the rate of change is around –2.11 D/year, which slows to –0.35 D/year by school age.
Here’s a breakdown of the median 5-year change in spherical equivalent refractive error across different patient groups:
| Patient Group | Median 5-Year Change in Refractive Error |
|---|---|
| Bilateral Aphakia | –8.38 D |
| Unilateral Aphakia | –10.75 D |
| Bilateral Pseudophakia | –1.63 D |
| Unilateral Pseudophakia | –1.94 D |
Pseudophakic eyes exhibit smaller shifts because the fixed power of the IOL does not adapt to the eye’s growth. Unilateral cases often end up more myopic by the 10-year mark (median –10.63 D) than bilateral cases (median –4.81 D). This difference arises partly because surgeons aim for less initial hyperopia in unilateral cases to better align with the fellow eye.
What Is Myopic Shift and How Does It Affect Long-Term Vision
Myopic shift refers to the gradual progression toward nearsightedness as the eye grows, while an implanted IOL remains static. This phenomenon significantly impacts long-term vision, especially in children who already face challenges like amblyopia and reduced visual acuity.
A long-term study of infants who received IOL implants before their first birthday found that all eyes experienced a myopic shift over an average follow-up of 15.9 years. By the 10-year point, the average shift was –11.62 D, with a range spanning from –3.75 D to –21.88 D. As one expert observed:
"Considerable variation in myopic shift hinders the prediction of long-term refractive outcomes in individual patients." – Joyce JT Chan, FRCOphth, Department of Ophthalmology and Visual Sciences, The Chinese University of Hong Kong
The age at surgery is a key factor in determining the extent of the shift. Children operated on before age 2 show an annual shift rate of approximately 0.84 D/year, compared to 0.24–0.28 D/year for those treated between ages 4 and 6. Even a decade after surgery, about 50% of eyes continue to show a myopic shift exceeding –2.00 D.
To account for this growth, surgeons often target mild to moderate hyperopia immediately after surgery. Evidence suggests keeping this target below +7.00 D, as higher levels of hyperopia are associated with poorer long-term visual outcomes:
"When selecting target refraction in infants, low to moderate hyperopia (<+7.00 dioptres) should be considered to balance the avoidance of high myopia in adulthood with the risk of worse long-term visual acuity related to high postoperative hyperopia." – Hong Kong Medical Journal
Frequent follow-ups are crucial, as both refractive error and visual acuity significantly influence long-term vision and quality of life. Given the unpredictable nature of the myopic shift, regular monitoring throughout childhood and adolescence ensures that optical corrections remain effective.
Complications and Follow-Up Surgeries
Long-term issues after pediatric cataract surgery often include glaucoma and visual axis opacification (VAO). These complications can arise years after the initial procedure, requiring ongoing care.
Glaucoma and Glaucoma Suspect Cases
Glaucoma is the most serious long-term risk of pediatric cataract surgery, and it can take years to manifest. In fact, cases have been documented as late as 16.5 to 17 years after surgery. Studies show the overall rate of secondary glaucoma is 33.33% (45 of 135 eyes). According to the Infant Aphakia Treatment Study (IATS), by the 10.5-year mark, 41% of children had developed glaucoma or were classified as glaucoma suspects.
The surgical approach to lens management plays a major role in glaucoma risk. For instance, the 5-year cumulative incidence of glaucoma-related complications is 46% in bilateral aphakia but only 7% in bilateral pseudophakia. However, as Dr. Scott R. Lambert, Principal Investigator at Stanford University, pointed out:
"The results challenge the notion that replacing the child’s lens with an implanted one protects the child from developing glaucoma, a belief among some pediatric ophthalmology surgeons."
Certain factors increase the risk of glaucoma, including bilateral aphakia, a corneal diameter under 9.5 mm, younger age at surgery, and a shallow anterior chamber depth before surgery (odds ratio 5.8). Dr. Sharon F. Freedman, a pediatric glaucoma specialist at Duke University, stresses the importance of regular follow-ups:
"Any child who has had a cataract removed needs to be seen by an eye care provider once a year at a minimum."
Children classified as glaucoma suspects should undergo evaluations every four to six months.
In addition to glaucoma, visual axis opacification is another common complication.
Visual Axis Opacification
Visual axis opacification occurs when a membrane or haze forms along the central visual pathway, impairing sight after surgery. Unlike glaucoma, VAO is more frequently observed in pseudophakic eyes – those with an implanted intraocular lens (IOL). Within five years, VAO develops in about 40% to 42% of pseudophakic eyes, compared to just 13% of aphakic eyes. Additionally, about one-third of pseudophakic eyes require a follow-up procedure to restore clarity within that timeframe.
When intervention is necessary, 64% of cases are addressed with Nd:YAG laser treatment, while 33% require surgical membranectomy or vitrectomy. Preventative measures, such as performing a primary anterior vitrectomy during the initial surgery, have proven effective. For children with Persistent Fetal Vasculature (PFV), this approach reduced VAO incidence from 60% to 15% and cut the need for additional surgeries from 46% to 19%. For children under age 8, combining a Posterior Continuous Curvilinear Capsulorhexis (PCCC) with a limited central anterior vitrectomy is now a widely accepted technique to minimize secondary membrane formation.
These complications highlight the importance of consistent, long-term follow-up care to ensure the best outcomes for pediatric patients.
Functional Outcomes and Quality of Life
Even after surgery, children can encounter functional challenges. Achieving successful surgical results often requires ongoing rehabilitation to improve daily activities, with consistent amblyopia treatment during early childhood being a key factor in long-term success.
How Better Vision Affects Daily Activities
Improved vision after surgery can significantly enhance a child’s ability to navigate daily life. Research using the Pediatric Eye Questionnaire highlights notable disparities in functional vision between children with cataracts and their peers. For instance, children aged 5–11 score 23 points lower in the Functional Vision domain (median 78 versus 100), while for younger children aged 0–4, the gap increases to 27 points (median 75 versus 100).
These vision challenges often translate into slower reading speeds, reduced physical activity, and academic difficulties. Additionally, other factors like motor skills and reading abilities can be further impacted. As noted in BMC Ophthalmology:
"Timely surgery alone is not enough to get good visual and motor outcomes in congenital cataracts. Adherence to visual rehabilitation, cataract laterality, and the presence of nystagmus were the three most critical things that affected the final visual acuity."
Children with bilateral cataracts tend to have better functional vision outcomes compared to those with unilateral cataracts. This is primarily because unilateral cases present a higher likelihood of severe amblyopia .
What Patients and Parents Reported About Long-Term Results
The impact of pediatric cataracts goes beyond vision, affecting the emotional and psychosocial well-being of both the child and their family. Parents of children aged 0–4 report significantly lower scores – 46 points lower, to be exact – on the "Worry about their Child’s Eye Condition" domain compared to parents of children without eye issues. Interestingly, research indicates that parents often feel a greater negative effect on health-related quality of life than the children themselves do.
Psychosocial challenges, such as visible eye misalignment or dependence on corrective devices, can further influence a child’s well-being, particularly during adolescence. These issues emphasize the importance of a long-term care approach that includes not just medical follow-ups but also emotional and psychosocial support. Comprehensive strategies are essential to address the full spectrum of recovery needs for both the child and their family.
Conclusion: Key Findings on 10-Year Pediatric Cataract Surgery Outcomes
Research highlights that timing is everything when it comes to pediatric cataract surgery. Children who undergo surgery within the first 90 days of life have the highest chances of achieving a visual acuity (VA) of 0.3 logMAR or better. For children with bilateral cataracts, implanting an intraocular lens (IOL) before 31 months significantly boosts outcomes, with a reported Hazard Ratio of 3.70. That said, early surgery isn’t without its challenges – it increases the likelihood of complications later on.
One of the most concerning risks is glaucoma. The 5-year cumulative incidence of glaucoma or being labeled as a glaucoma suspect is 46% in children with bilateral aphakia. Even more worrying, new cases of glaucoma have been identified as late as 17 years post-surgery. Melissa Murphy and her colleagues at Temple Street Children’s University Hospital emphasize the importance of ongoing care:
"It can occur up to 17 years post cataract surgery, evidence that long-term follow-up is imperative."
Another common issue is visual axis opacification, especially in pseudophakic eyes. Within five years, approximately 1 in 3 children will need additional surgery to address this. Long-term visual acuity often stabilizes by age 7, making this an important checkpoint for assessing future outcomes.
Achieving the best results requires more than just timely surgery. Comprehensive care, including strict visual rehabilitation, consistent monitoring for late complications, and emotional and practical support for families, plays a crucial role. These findings underline the importance of both early intervention and ongoing follow-up. Collaborating with experienced specialists, like those at Boulder Eye Surgeons, ensures children receive personalized care tailored to their unique needs.
FAQs
How do I know if my baby has a cataract?
Parents might spot cataracts in infants during routine checkups or by observing certain signs, such as leukocoria (a white or cloudy appearance in the pupil), strabismus (eyes that seem misaligned), or nystagmus (involuntary, rapid eye movements). Detecting these issues early is essential for proper vision development. If you’re worried about your child’s eye alignment or appearance, it’s important to seek professional advice quickly. Boulder Eye Surgeons provides comprehensive pediatric eye exams and tailored care for families in Boulder, CO, and surrounding communities.
Will my child need glasses or contacts long term after surgery?
Whether your child will need glasses or contact lenses over the long term depends on their unique vision requirements. For children who are aphakic (missing the natural lens inside the eye), glasses or contact lenses are often used as their eyes develop. Even if an intraocular lens is implanted, glasses might still be necessary to achieve the best possible vision. At Boulder Eye Surgeons, the team provides tailored care to create a vision correction plan that meets your child’s individual needs.
What warning signs of glaucoma should parents watch for after surgery?
An increase in intraocular pressure can be an early indicator of glaucoma following pediatric cataract surgery. Since children may not be able to complete visual field tests, consistent follow-up appointments with an eye specialist are essential. At Boulder Eye Surgeons, we emphasize the importance of regular monitoring because glaucoma can appear soon after surgery or even years later. Parents should remain vigilant, as the condition often develops without noticeable symptoms.



