
Pediatric cataracts can impair a child’s vision, but early diagnosis and timely surgery can prevent long-term issues like lazy eye or vision loss. Unlike adult cataract surgery, the procedure for children is more complex, requiring general anesthesia and careful post-surgery care. Here’s what you need to know:
- Causes: Genetics, infections during pregnancy (e.g., Rubella), trauma, or medical conditions like Down syndrome.
- Symptoms: White pupil (leukocoria), poor face tracking, nystagmus (eye shaking), or strabismus (crossed eyes).
- Surgery Timing: For congenital cataracts, surgery is often recommended within the first 4–6 weeks of life.
- Treatment Options: Intraocular lenses (IOLs), contact lenses, or glasses, depending on the child’s age and needs.
- Recovery: Involves protective shields, eye drops, and patching therapy to prevent lazy eye.
Early intervention, consistent follow-ups, and rehabilitation are key to improving a child’s vision after surgery.
Causes and Symptoms of Pediatric Cataracts
Common Causes of Pediatric Cataracts
Understanding what causes pediatric cataracts is a key step in managing the condition. One of the main causes is genetic mutations, especially in cases where both eyes are affected. In fact, autosomal dominant inheritance is responsible for 44% of bilateral cataracts. This means a child can inherit the condition even if only one parent carries the gene. Genetic testing has become incredibly precise, identifying specific mutations in up to 90% of bilateral cases. This information not only helps doctors create better treatment plans but also provides families with insights for future planning.
Cataracts can also result from infections during pregnancy, known as TORCH infections. These include Toxoplasmosis, Rubella, Cytomegalovirus (CMV), Herpes simplex, and Syphilis. Among these, Rubella is preventable with vaccination. Another common cause is ocular trauma, which accounts for 12% to 46% of unilateral cataracts in children. Additionally, cataracts may be linked to broader medical conditions like Down syndrome, Alport syndrome, and metabolic disorders such as galactosemia.
It’s worth noting that about 15% of inherited congenital cataracts occur alongside systemic syndromes. This is why a diagnosis often involves not just an eye specialist but also a pediatrician and a geneticist.
Signs Parents Should Watch For
Some signs of pediatric cataracts are visible, while others are more subtle. A key physical indicator is leukocoria, a white or gray pupil that might be noticeable in flash photographs, where one pupil appears white instead of red. If you see this, it’s important to consult a doctor immediately.
Behavioral signs can also point to vision problems. For example, infants who aren’t tracking faces by 3–4 months may have an issue. Older kids might hold objects unusually close, bump into things, or report double vision or faded colors. Other symptoms include nystagmus (a rhythmic shaking of the eyes) and strabismus (misaligned or crossed eyes).
"If you get the sense that your baby isn’t seeing and responding, that may be a tip off that something is wrong." – Boston Children’s Hospital
Here’s a quick summary of what to watch for:
| Category | Signs to Look For |
|---|---|
| Physical Signs | White or gray pupil (leukocoria), cloudy lens |
| Eye Movements | Nystagmus (shaking eyes), strabismus (crossed eyes) |
| Visual Behavior | Poor face tracking by 4 months, frequent bumping, holding items very close |
| Sensory Complaints | Double vision, faded colors, light sensitivity, glare |
These signs should prompt further investigation through routine vision screenings.
How Vision Screening Works
Early detection is critical. Pediatricians perform a red reflex test immediately after birth and during well-child visits. This involves shining a light into the baby’s eyes to check for a healthy reddish-orange reflection. If the reflection appears white, gray, or uneven, it could indicate a cataract.
When abnormalities are detected, the child is referred to a pediatric ophthalmologist for a more detailed evaluation. This includes a dilated eye exam and, if needed, an ocular ultrasound to assess the cataract’s density and confirm the retina’s health. Timing is everything – surgery for dense cataracts is most effective when performed within the first 4–6 weeks of life.
"Visual prognosis is closely linked to the timing of intervention, cataract density, and adherence to follow-up care." – Arkaprava Ray and Bharat Gurnani, StatPearls
sbb-itb-c87b093
Deciding on Surgery
When Is Surgery Necessary?
After diagnosing a pediatric cataract, the next step is determining whether surgery is required. Surgery is typically reserved for cataracts that are large enough or positioned in a way that interferes with normal development of the eye and brain connection. A cataract located centrally and measuring more than 3 mm in diameter is generally considered to affect vision significantly, making surgery necessary.
Smaller cataracts, especially those located at the edge of the lens or outside the main visual axis, may not require immediate intervention. If the child’s vision is developing normally, these cataracts are often just monitored. However, when surgery is needed, timing is critical to prevent amblyopia (commonly known as lazy eye). For unilateral cataracts, surgery is usually performed between 4 to 6 weeks of age, and for bilateral cases, between 6 to 8 weeks.
"Children may lose vision permanently because of amblyopia (lazy eye) if a severe cataract is not removed quickly." – Boulder Eye Surgeons
Once the timing is determined, the next step involves thorough preoperative planning.
Preoperative Planning
Before surgery, a detailed evaluation is conducted, often including an Examination Under Anesthesia (EUA). This allows the medical team to take precise measurements of the eye and assess the retina. One of the most critical measurements is the axial length, which helps determine the appropriate lens power. This is particularly important because a child’s eye grows significantly – from about 16.5 mm at birth to roughly 23 mm by age 13 – making lens power calculations more complex.
During this stage, parents will discuss lens options with the surgeon. Choices typically include intraocular lenses (IOLs), contact lenses, or glasses. For infants under one year old, contact lenses are often preferred because they can be adjusted as the eye grows. IOLs, while more convenient for older children, are permanent and carry a higher risk of complications such as glaucoma and uveitis in very young patients. Glasses are usually used as a supplemental option when other methods are not practical.
| Lens Option | Best For | Key Consideration |
|---|---|---|
| Intraocular Lens (IOL) | Older children (typically 2+) | Permanent; less adaptable to eye growth |
| Contact Lenses | Infants under 1 year | Adjustable; requires daily care from parents |
| Glasses | Any age as a supplement | May distort image size; not ideal as a standalone solution |
Questions to Ask Your Surgeon
Being well-prepared for your consultation can make a big difference. Since early intervention is crucial, you’ll want to ensure you understand the specifics of your child’s condition and the proposed treatment. Here are some key questions to consider asking your surgeon:
- Is this cataract visually significant? Ask for a clear explanation of how the cataract’s size and location impact your child’s vision and whether surgery is necessary.
- What’s the optimal timing for my child’s case? Timing may differ depending on whether the cataract is unilateral or bilateral, so request a tailored recommendation.
- What lens option do you recommend, and why? Discuss how the surgeon plans for future eye growth when choosing the lens power.
- What does post-surgical rehabilitation involve? Learn about amblyopia therapy and the follow-up care required after surgery.
- What are the risks of secondary complications? Since about 20% of children develop secondary glaucoma after cataract surgery, it’s important to understand the need for long-term monitoring.
- How many pediatric cataract surgeries do you perform annually? Pediatric eyes differ significantly from adult eyes, so experience with these surgeries is essential.
- If the cataracts are bilateral, should I consult a geneticist? Ask if a referral is needed to check for underlying conditions like galactosemia or other systemic disorders.
These questions can help you feel more informed and confident about your child’s treatment plan.
Pediatric Cataracts: Diagnosis, Treatment and Future Implications
The Pediatric Cataract Surgery Process
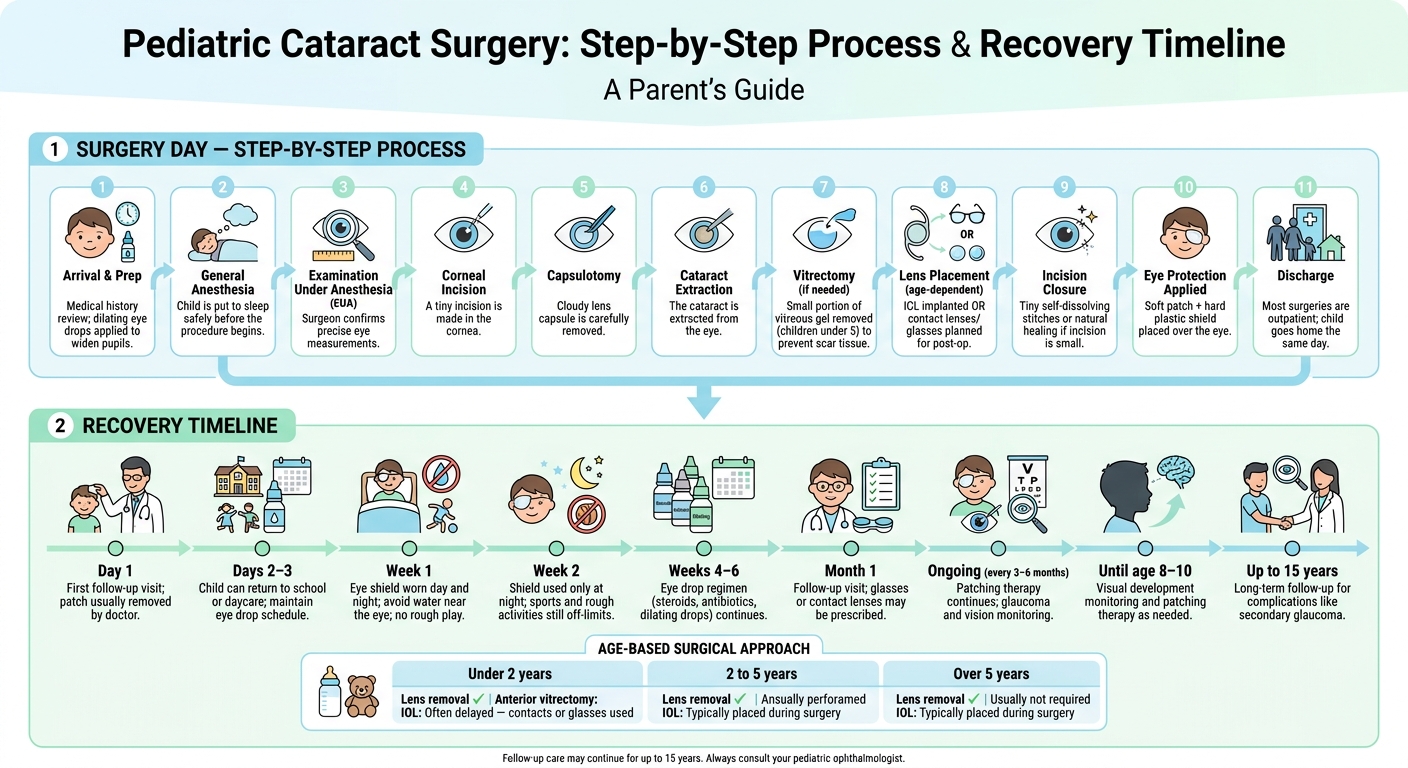
Pediatric Cataract Surgery: Step-by-Step Process & Recovery Timeline
What to Expect on Surgery Day
Surgery day can feel like a whirlwind, but understanding the steps ahead can make it much smoother. When you arrive, the medical team will go over your child’s medical history and apply dilating eye drops to prepare the eyes for surgery. These drops help widen the pupils, a necessary step before general anesthesia is given. Once your child is asleep, the surgeon will perform a final exam under anesthesia (EUA) to confirm the exact measurements needed for the procedure.
Most pediatric cataract surgeries are done as outpatient procedures, meaning your child can typically head home the same day. After these initial preparations, the operation begins with a series of precise, carefully executed steps.
How the Surgery Works
The surgery starts with the surgeon making a tiny incision in the cornea. From there, they perform a capsulotomy (removing the cloudy lens capsule) and extract the cataract. For children under 5, a small portion of the vitreous gel may also be removed to prevent scar tissue from obstructing vision later. Depending on the child’s age, an intraocular lens (IOL) may be implanted during the procedure, or the child may use contact lenses or glasses until an IOL can be placed.
The surgical approach varies by age group, as shown in the table below:
| Age Group | Lens Removal | Anterior Vitrectomy | IOL Placement |
|---|---|---|---|
| Under 2 years | Yes | Usually performed | Often delayed; contacts or glasses used |
| 2 to 5 years | Yes | Usually performed | Typically placed during surgery |
| Over 5 years | Yes | Usually not required | Typically placed during surgery |
After the cataract is removed and any necessary lens adjustments are made, the surgeon closes the incision with tiny, self-dissolving stitches or allows it to heal naturally if the cut is small enough. To protect the eye after surgery, a soft patch and a hard plastic shield are placed over it.
Risks and Possible Complications
Even with the utmost care, no surgery is completely without risks.
"Cataract surgery with a skilled surgeon is generally very safe. However, like any surgery, there are risks. These include infection, inflammation, glaucoma (increased eye pressure), issues with the retina and needing future eye procedures." – Children’s Hospital Colorado
One of the most serious long-term risks is glaucoma, which can develop months or even years after the surgery. This makes regular follow-up appointments critical. Inflammation, or uveitis, is another common post-surgery issue, which is why doctors often prescribe steroid eye drops to reduce swelling in the days following the procedure. Other potential complications include infections, retinal detachment, and visual axis opacification (VAO). VAO occurs when scar tissue clouds the visual path again, though surgeons now prefer sharp-edged IOLs, which have been shown to lower the chances of this happening compared to round-edged lenses.
While the surgery itself is a major step, it’s just the beginning of a longer journey in vision care. Regular monitoring and follow-ups are essential to ensure the best possible outcome for your child’s vision.
At Boulder Eye Surgeons, we are committed to following every step of this process with precision and care to support your child’s recovery and vision health.
Recovery and Long-Term Care
After surgery, careful recovery and ongoing attention are crucial to achieving the best possible vision results.
Care Right After Surgery
Right after the procedure, it’s important to keep a close eye on your child. Their eye will be covered with a soft patch and a hard plastic shield. The shield should stay on continuously for the first week, and then only at night during the second week to prevent accidental rubbing or injury.
At home, you’ll need to manage a routine of eye drops, which typically includes steroids to reduce inflammation, antibiotics to prevent infection, and dilating drops to aid healing. This regimen usually lasts 4 to 6 weeks, so staying consistent is essential. When applying drops, avoid putting pressure on the eyeball.
Keep the area around the eye clean using cooled, boiled water, and make sure your child doesn’t rub or touch their eye. Activities like swimming, immersing the eye in water during baths, or using hot tubs should be avoided for at least two weeks. Similarly, rough play and sports are off-limits during this time.
Be alert for signs like increased redness, cloudiness or a white appearance in the front of the eye, or excessive tearing. If you notice any of these, contact your surgical team immediately.
| Recovery Timeline | Key Guidelines |
|---|---|
| Day 1 | First follow-up visit; patch is usually removed by the doctor. |
| Days 2–3 | Child can return to school or daycare; maintain eye drop schedule. |
| Week 1 | Eye shield must be worn day and night; avoid water near the eye. |
| Week 2 | Use shield only at night; no sports or rough activities. |
| Month 1 | Follow-up visit to check healing; glasses or contact lenses may be prescribed. |
Vision Correction and Rehabilitation
While surgery removes the cloudy lens, clear vision doesn’t return immediately. For infants, contact lenses are often used because their eyes grow quickly and need adaptable solutions. Older children may receive an intraocular lens (IOL) implant during surgery, but many will still need glasses – often bifocals – for near vision support.
A key part of recovery is patching therapy (occlusion therapy). This involves covering the stronger eye for several hours daily to encourage the brain to rely on the operated eye, helping to prevent amblyopia (lazy eye). As explained by the University Children’s Eye Center:
"Cataract surgery is just the first step to improving vision. Connections between the eye and brain must be rebuilt."
The duration and schedule for patching vary by child and often continue until visual development is complete, usually around 8 to 10 years old.
Consistent rehabilitation is crucial, along with regular monitoring in the weeks and months that follow.
Follow-Up Appointments and Monitoring
Follow-up appointments are typically scheduled for 1 day, 1 week, and 1 month after surgery, with periodic visits continuing until visual development concludes (around age 8–10). During these visits, doctors check for infections, monitor for visual axis opacification (a type of scarring that can cloud vision again), and screen for glaucoma by measuring eye pressure.
"The risk of glaucoma is perhaps the most serious for kids undergoing pediatric cataract surgery, especially those at a younger age." – University Children’s Eye Center
With proper vision correction and consistent follow-up care, many children achieve vision levels between 20/60 and 20/100, with some even approaching normal sight.
At Boulder Eye Surgeons, we’re committed to guiding families every step of the way – from the first post-op visit to long-term monitoring – to help ensure the best possible outcomes for your child’s vision. This comprehensive care plan, combined with rehabilitation efforts, forms the foundation for successful recovery after pediatric cataract surgery.
Supporting Your Child Through the Vision Journey
Surgery is just one part of the process; ensuring your child’s vision develops properly requires ongoing care. This includes sticking to patching schedules, maintaining optical corrections, and attending regular follow-ups – every three months for infants and every six months for older children. These steps are critical to monitor progress and support the best possible outcomes.
As highlighted by BMC Ophthalmology:
"Timely surgery alone is not enough to get good visual and motor outcomes in congenital cataracts."
The journey doesn’t end after surgery. Complications can emerge over time, such as secondary glaucoma, which affects about 11% of unilateral cases, or postoperative strabismus, seen in up to 62% of unilateral cases. Because of these risks, a skilled care team may follow your child for as long as 15 years to ensure their vision remains stable.
Beyond the initial recovery, coordinated, long-term care becomes essential. A multidisciplinary team ensures that every aspect of your child’s vision journey is handled with precision. This approach builds on the surgical and post-operative strategies discussed earlier. At Boulder Eye Surgeons, they emphasize their commitment to individualized care:
"Our goal is to provide professional, compassionate and customized eye care to every patient, every time."
Since 1997, their team has worked tirelessly to support children through the entire rehabilitation process. As BMC Ophthalmology reiterates:
"Early diagnosis, well-planned surgery, and long-term care that is tailored to each person’s needs are all necessary for the best results."
FAQs
Will my child need more eye surgeries later?
Your child might require further procedures as they grow. Although cataract surgery works well, ongoing monitoring is crucial to manage potential complications like glaucoma, inflammation, or scar tissue. As their eyes continue to develop, additional surgeries – such as adjustments to eye muscles – might also be necessary. At Boulder Eye Surgeons, specialized follow-up care is available to address these changes and ensure your child’s vision remains on track throughout their development.
How do I choose between an IOL, contacts, or glasses?
When deciding between an intraocular lens (IOL), contact lenses, or glasses for your child, their age and specific needs play a big role. For kids older than two, IOL implantation is typically the go-to choice. However, for infants under six months, contact lenses or glasses are often recommended. This is because their eyes grow quickly, and there’s a higher risk of complications with IOLs at that age. At Boulder Eye Surgeons, consultations are tailored to evaluate the best option for your child’s vision and overall eye health.
How long will patching last after cataract surgery?
After surgery, your child will typically wear an eye patch and a protective shield. These are usually removed during the post-operative appointment the following day. In some cases, additional patching therapy may be required to ensure the operated eye develops as it should. The length of this therapy varies based on your child’s needs, but it often continues until at least age 6. Some specialists may suggest extending it up to age 9.



